


Despite the fact that a record 107,000 Americans died of fatal drug overdoses last year, patients in need of treatment are forced to navigate a punishing gauntlet to get the care they need, a group of addiction medicine specialists from Oregon Health & Science University argue in a new publication.
“Most people who need and want treatment for opioid addiction cannot access it,” they write in a perspective published in the Journal of General Internal Medicine.
The co-authors include OHSU’s Honora Englander, M.D., professor of medicine (hospital medicine and general internal medicine and geriatrics); Ximena Levander, M.D., M.C.R., assistant professor (general internal medicine and geriatrics); and Jessica Gregg, M.D., Ph.D., chief medical officer of Fora Health Treatment & Recovery in Portland and an associate professor of medicine in the OHSU School of Medicine.
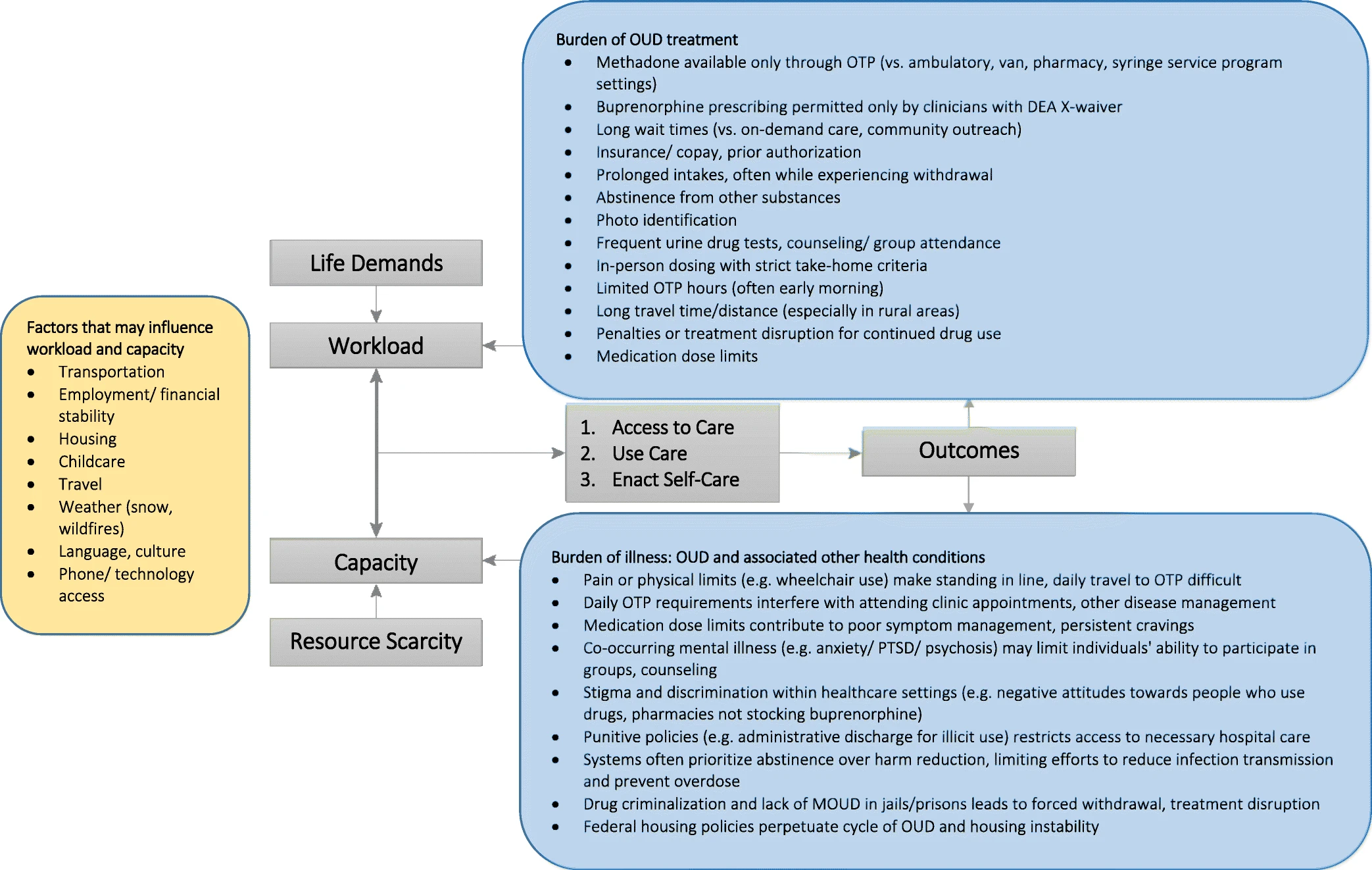
They describe the current system as “maximally disruptive care.”
To access medication for opioid use disorder — the gold standard for effective treatment — people must make daily visits to methadone clinics to get treatment, or they must find a clinician with a federal waiver to prescribe buprenorphine. Those with complicating medical conditions typically find little help, and they’re often faced with enormous treatment burdens, including having to stand in line just to receive medication the day after being discharged from the hospital for life-threatening illnesses.
“Maximally disruptive care for opioid addiction is not an accident,” they write. “Rather, demands on patients are part of the treatment paradigm. Patients must ‘earn’ methadone take-home doses or ‘work the steps’ to be worthy of treatment.”
Englander cited the example of one recent patient who was admitted to OHSU Hospital with a high-risk pregnancy.
OHSU’s Project IMPACT, the in-hospital addiction team that Englander leads, connected with the patient because of her addiction to fentanyl — a cheap and potent opioid that has surged into Oregon and the nation over the past two years. The patient was highly motivated to stop using the drug and needed methadone, a medication that reduces opioid cravings and treats opioid use disorder. Because she was pregnant, she needed methadone in the morning and evening.
Yet, to get treatment after discharge she would have to travel to a clinic, a 45-minute drive from her home on the Oregon coast.
That’s because federal regulations established in 1971 require methadone to be dispensed through a federally certified opioid treatment program. Federal regulators eased those regulations during the COVID-19 pandemic, but a nationwide survey published by Levander and co-authors a year ago reveal that many opioid treatment program leaders nonetheless continue to resist easing access.
For Englander’s patient on the coast, the requirement was insurmountable because she didn’t have a car.
“Even if she did have a car, that’s three hours of driving every day,” Englander said. “She wanted to be off fentanyl; she wanted to be a healthy parent. Imagine having to travel to a methadone clinic 1 ½ hours roundtrip twice a day while pregnant or days after delivering your baby just to receive the treatment that allows your family to be healthy.”
To reduce these barriers, the authors call for a minimally disruptive approach that would create flexible, adaptive, context-sensitive, individualized, coherent and holistic treatment options for opioid use disorder.
“Minimally disruptive medicine is a framework that focuses on achieving patient goals while imposing the smallest possible burden on patients’ lives,” the authors write. Programmatic and policy changes, they argue, could “begin to address disparities and inequities, and save lives.”